
Prior to embarking on any fertility treatment, it is invaluable to be able to predict an outcome. This heavily depends on the woman’s ovarian reserve, which is most reliably determined by the female age.
At age 20, only approximately 2.4% of sexually active women cannot achieve a live birth. However, by age 40, 35% of women have troubles falling pregnant. This increases sharply to 50% at the age of 41 and 90% at the age of 45.
The impact of age is two-fold: there is a progressive depletion of the number of fertilisable eggs, which is also accompanied by an age-related decrease in quality.
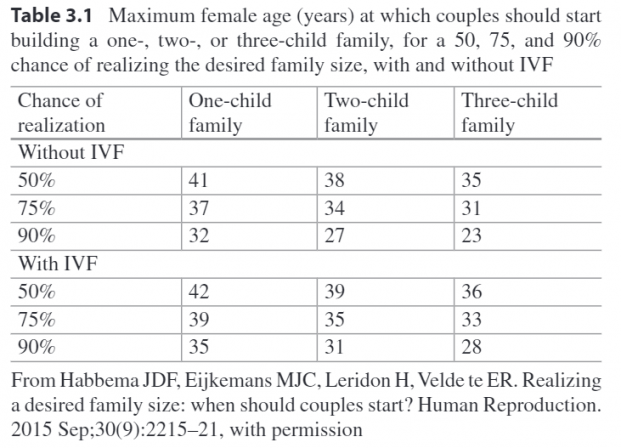
Since advancing age is not reversible, it is a good idea for couples to plan ahead how many children they would like to have and when. If you are willing to go through assisted reproductive technologies, it may be acceptable to delay childbearing for a few years. However, there is always the possibilities that things may not go as planned. The following table can be used as a general guideline for the latest female age to start building a family of certain size, with or without IVF.
Ovarian reserve testing
A more personalised and accurate strategy for family planning is to test the ovarian reserve. The most common ovarian reserve test in the clinic nowadays involves checking the levels of Anti-Müllerian hormone (AMH).
AMH is described as the “follicular gatekeeper” that limits the size of the follicle cohort available to respond to hormonal signals each month. Since AMH is only produced by follicles at the later stages of development, they represent a “functional” pool of the ovarian reserve.
Women with a very low AMH level can be predicted to produce a low number of fertilisable eggs upon controlled ovarian stimulation, which dramatically reduces the efficiency of IVF treatment. In these women, the conventional stimulation protocol may not be helpful for the purpose of producing multiple eggs per cycle.
In addition, AMH has recently been proposed as a biomarker for optimising the dosage of ovarian stimulating drugs. It has proved to be a great predictor for ovarian hyperstimulation, a life-threatening condition associated with gonadotrophin stimulation.
What can women do to “stop” the ticking clock?
One way to plan for the future is to freeze eggs or embryos at a younger age. Ideally, eggs should be retrieved before 30 and definitely before 35. This is because both the quantity and quality of eggs that can be retrieved per cycle plummet after mid-30s.
While frozen transfers are frequently successful nowadays, the use of egg freezing is by no means a safeguard option against age-related fertility decline. Women of advanced maternal age are also more likely to have other conditions that increase the risk of adverse pregnancy outcomes, independent of egg quality itself.
Importantly, women should avoid multiple pregnancies and only undergo single embryo transfer to ensure safety. Since age is also correlated with increased genetic mistakes known as aneuploidy. preimplantation genetic screening for aneuploidy is highly recommended to select chromosomally normal embryos.
Takeaways:
- Couples may consider fertility evaluation testing, especially AMH test for ovarian reserve, as part of family planning or before fertility treatment.
- Woman at advanced reproductive age should be aware of the risks of poor ovarian response, reduced egg retrieval and fertilisation rates.
- Woman at advanced reproductive age are encouraged to be evaluated for other comorbidities that may complicate the pregnancy.
- In women above the age of 40 with a low AMH level, egg donation may be discussed as an alternative.
For more personalised information regarding fertility preservation and treatment, you can contact Melbourne-based specialist, Dr Alex Polyakov here.