
Men’s sexual health is often a difficult conversation because of the stigma associated with reduced masculinity, but it’s nonetheless one that needs to be had.
Androgen deficiency occurs when male hormones are low, which primarily concerns the hormone testosterone. However, its symptoms often go under the radar and even a confirmed diagnosis can be frequently overlooked.
What is testosterone and testosterone deficiency?
Testosterone is the major androgen that is critical for male infertility as it acts on cells in the testes to make sperm. Apart from a well-known fertility function, it also contributes to development of the male reproductive organs, puberty features, bone and muscles, sex drive and general mood.
Testosterone deficiency occurs 1 in 200 men under the age of 60 and 1 in 10 men over 60 years old. As men age, the testosterone levels gradually decrease at a rate of approximately 1% per year starting in the late 30s. This decline may be accelerated if a man is overweight or have chronic health conditions.
Warning signs of low testosterone
Symptoms of low testosterone can overlap with other illnesses, such as mood swings, irritability, poor concentration and low libido. At different ages, the exact symptoms also vary. For example, small children with low testosterone generally have small penis and testicles. Teenagers can experience late or abnormal puberty. Adults can experience a wide range of symptoms, including:
- Reduced muscle strength
- Difficulties with erection
- Hot flushes, sweats
- Female-type breasts
- Increased body fat
- Irritable mood, poor concentration
- Lethargy
- Low set drive
For more complete descriptions of the symptoms at each age group, you can visit Healthy male.
Causes of testosterone deficiency
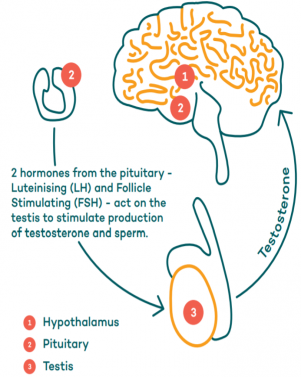
The most common cause of testosterone deficiency is a genetic condition called the Klinefelter syndrome, which affects 1 in 550 men. Since testosterone production involves the hypothalamus and pituitary in the brain, as well as the testis, a problem in any of these organs can jeopardise testosterone production.
Source: Healthy male
In addition, some medical conditions and medications can cause androgen deficiency, which may resolve once the medical condition is treated or medication is stopped. These include:
- Infections by mumps after puberty
- Cancer treatment, especially testicular cancer
- Clinical depression
- Long-term opiate therapy
How is testosterone deficiency diagnosed?
Although having symptoms may be a warning sign of low testosterone, they could also be caused by other health problems. Thus, diagnosing testosterone deficiency requires measuring the hormone levels on least on two separate days and detecting lower than normal hormone levels. Patients will also need to undergo a full medical examination to find out potential causes.
Treatment
A diagnosed testosterone deficiency is treated with testosterone therapy that usually continues for life. In Australia, testosterone therapies are available in the forms of injections, gels, creams, patches and tablets. However, if you are diagnosed with both diabetes and testosterone, treating diabetes first might restore your testosterone levels.
In 2015, the PBS criteria for testosterone prescription changed so that the patient is only eligible for subsidised prescriptions after consulting with an endocrinologist, urologist or member of the Australasian Chapter of Sexual Health Medicine. After this change, it is estimated that only 50% of patients with testosterone deficiency commenced a PBS-subsidised treatment and 24% of patients do not commence therapy due to the cost or inconvenience.
The prescription rules were tightened because testosterone replacement therapy in older men with only modest testosterone declines was controversial. The testosterone decline in this group of patients is usually linked with another chronic illness or obesity. The benefits and risks of testosterone treatment for them are not yet clear. The Endocrine Society of Australia explained that “There are limited data from high-quality randomised controlled trials with clinically meaningful outcomes to justify testosterone treatment in older man, usually with chronic disease…”
Androgen deficiency is generally not life-threatening, and many undiagnosed men do live without treatment. Having said that, the life quality of men with untreated androgen deficiency may be lower, as low testosterone raises the risk of developing conditions like osteoporosis. Outside the PBS scheme, your GP can still prescribe testosterone therapy on a private script and monitor your treatment.
Bottom line
If you think that you are experiencing symptoms related to testosterone deficiency or having difficulty conceiving, raising the concern with your GP or fertility specialist is important. You can find out more about androgen deficiency in this booklet by the Healthy Male, or contact a fertility specialist like Dr. Alex Polyakov for a personalized consultation. Get in touch online or on 0394860677 to ask your questions.
Information on restarting fertility treatment
Good news! The government has lifted the ban on IVF and elective surgeries in late April. We acknowledge the disappointment that many patients would have felt during the delay for fertility treatments and would like to extend a warm welcome back to you all.
Although the pandemic is not over yet, Australia has done well in flattening the curve in a timely manner. Therefore, we are delighted to be able to help complete families again!
In line with the government’s directive to lift restrictions in an incremental way to avoid risks, Melbourne IVF follows the suggested approach for elective surgery, including:
- Perform 50% of the original workload in first two weeks
- Prioritise patients with more urgent cases
- Physical distancing is applied in the lead up and management of treatment where appropriate, such as using telehealth and limiting face to face contact to less than 15 minutes
- Test patients for temperature or COVID-19 where appropriate
- Increased hygiene and infection control measures in the clinic
Who will be treated first?
We are fully committed to treat all of our patients. But in the first few weeks of reopening, we will have to prioritise more urgent cases. According to the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG), compelling reasons for medical management are first considered, including heavy menstrual bleeding, pelvic pain, endometriosis.
With regards to IVF treatment, we will also determine the state of urgency based on criteria like the woman’s age and her egg reserve. You may already know that a woman’s fertility and IVF success rate decline with age, most drastically after 35 years old. This is because a woman is born with all the eggs she will ever have, which makes egg reserve a critical determinant for her fertility.
The Anti Mullerian Hormone (AMH) test gives an indication of the remaining egg reserve and fertile years. As such, women who are older and have low egg reserve will be prioritsed over other non-urgent procedures. For example, fertility preservation for social reasons in a younger woman is most likely to be considered non-urgent. An exception to this is fertility preservation due to upcoming cancer treatment.
Is it riskier to get pregnant now?
So far, research findings on COVID-19 and its effects on fertility do not indicate increased risks of pregnancy complications or harm to newborn babies. Nevertheless, we don’t know for sure yet and it’s always good to take some precautions. Having a fever in the first trimester is known to have negative consequences regardless whether it’s caused by COVID or a seasonal flu. Therefore, if you have a fever, we advise you to stay home and begin an IVF cycle at a later cycle. Please also be sure that you have received a flu vaccine.
It is worth nothing that a recent study published in JAMA Network Open reported the presence of coronavirus in a proportion of male patients who have recovered or are currently infected with COVID-19. Therefore, if you or your partner suspect a recent COVID-19 infection, please be sure to inform your doctor.
Egg, sperm donation and surrogacy options in Australia
Seeking egg, sperm donations or surrogacy arrangement in overseas countries with more relaxed rules was a popular option for Australian couples before quarantine. Unfortunately, fertility abroad is not really a viable solution due to the current pandemic that needs no introduction.
Here in Australia, we have done exceptionally well in flattening the curve, which led to a lift in the ban on IVF and other elective surgeries. However, in Europe and the United States, such bans are still in place as the COVID-19 situation is nowhere near as promising. Another hurdle at the moment is the international travel restrictions that are unlikely to be eased in the near future.
Therefore, if you are considering IVF, donor treatment or surrogacy this year or next year, staying in Australia will likely give you a better chance. In addition to a lower risk of catching COVID and avoiding some travel fees, the Victorian Assisted Reproductive Treatment Authority (VARTA) lists a number of benefits associated with using an Australian donor or altruistic surrogate:
- Ensure thorough preparation of all parties
- Have support from local family and friends
- Experience fewer legal challenges regarding immigration and citizenship
- Potentially maintain ongoing communication with the surrogate if desired
- You are more likely to find partners with similar values, culture and language.
- Often cheaper and more convenient
In the past, there was a shortage of egg/sperm donors in Australia, but this has been significantly improved. In the past year, over 220 women in Victoria donated eggs, and only 10% of frozen eggs are currently used for IVF in Australia, leaving much room for donation.
Melbourne IVF’s donor programme follows the Victorian donation laws, which is supported by the managing body VARTA. Some core rules in place to protect you include:
- A limit of 10 women can be treated by the same donor under Victorian rules, avoiding a large number of potential relatives
- It is an offence for surrogates and donors to receive payment for donation other than covering the travel and medical expenses
- Donor-conceived Victorians from egg, sperm or embryo donation can access identifying information about their genetic origin
Navigating the journey of assisted reproductive treatment can be challenging, especially when complex legislations are involved. Fortunately, there are experienced counsellors who can assist you on fertility and donor conception issues. Melbourne IVF also has its own counselling team that can be reached on (03) 9473 4418.
Egg and sperm donation
In some couples with infertility, egg or sperm donation is needed to complete a family if:
- The woman has gone through a premature menopause
- There is a risk of passing on a genetic disease in either partner
- The woman’s ovaries are affected by cancer treatment or other serious illness
- You have tried IVF treatment, but repeated cycles failed due to poor egg/sperm quality
There are three ways to find an egg or sperm donor. One is using a clinic donor who has been recruited by the clinic and medically screened. For example, Melbourne IVF’s egg donation program recruits local donors between 25-35 years old with around 5-10 donors available each year.
Although you don’t personally know the clinic donor, all donors need to consent to their identifications being released to the person created when they turn 18. The donors may also indicate that they are open to being contacted before the child becomes an adult.
Another option is to use a known donor, who could be your family member, friend or an acquaintance. When using a known donor, you have the chance to interact with him/her more, which you may find desirable.
Lastly, you can also advertise for a donor after gaining approval from the Health Minister. For more information regarding the three options, you can visit “Finding a donor” by VARTA.
Domestic surrogacy
Surrogacy in Australia is a viable option for couples due to these reasons:
- A woman is unable to become pregnant or carry a baby due to uterine problems, risks of pregnancy complications and other existing health problems
- Recurrent miscarriage and repeated IVF failures
- A same-sex couple or individual who want to have a child conceived through donor sperm or egg
- A male partner may commission a surrogate to give birth to a child using frozen embryos from a deceased female partner
In Victoria, commercial surrogacy involving payment to the surrogate is illegal and traditional surrogacy in which the surrogate mother uses her own egg is also not permitted in fertility clinics. The only type of surrogacy permitted in Victorian clinics is gestational surrogacy, meaning that the surrogate mother has no genetic link to the baby but simply carries out the pregnancy. Although the surrogacy must be altruistic, you do need to cover the surrogate’s expense during pregnancy and birth.
Before finding a surrogate mother, the first step is to ensure that both you and your partner are emotionally ready for what is involved. As such, you are recommended to contact a fertility clinic counsellor for advice. You may also find useful advice from the support group Surrogacy Australia.
Finding a surrogate may start by asking your family members, or through your networks. Note that it is illegal to advertise for a surrogate. When in doubt, please seek professional advice. The brochure on “Finding a surrogate” is a great resource from VARTA.
Bottom line
To sum up, although the COVID-19 pandemic may have disrupted your plan to have a baby abroad, there are still plenty of options within Australia. For more personalised information regarding donor programmes or surrogacy, you can contact Melbourne-based fertility specialist, Dr Alex Polyakov here.